A 64-year-old woman with dilated right pupil, nausea, and headache
Article Sidebar
Main Article Content
Abstract
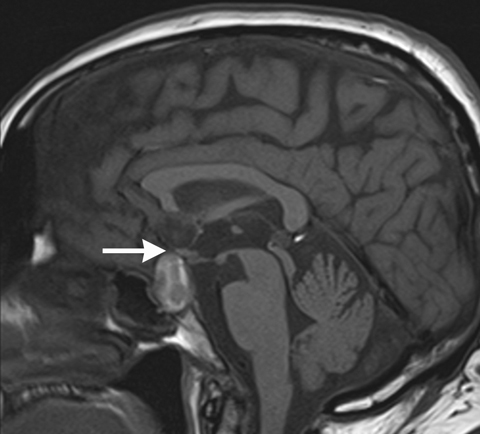
A 64-year-old woman presented with a dilated right pupil and nausea that began 3 days after the onset of a mild but constant headache. She complained of an inability to focus but had no loss of vision and reported no diplopia in primary gaze. There was associated photophobia but no neck stiffness. She had completed 2 weeks of therapeutic enoxaparin for a right below-knee deep vein thrombosis (DVT), diagnosed a month prior. Anticoagulation medication was prescribed after a follow-up scan at 2 weeks showed minimal residual DVT in a branch of the medial gastrocnemius vein along with partial resolution of the thrombus in the greater saphenous vein. The patient’s medical history was remarkable for hypothyroidism, but she did not suffer from hypertension, diabetes, or cardiovascular disease. She had noticed a gradual weight gain over the preceding year, and her primary care physician began testing free urinary cortisol 2 weeks prior to presentation.
Downloads
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.




References
Turgut M, Özsunar Y, Basak S, et al. Pituitary apoplexy: an overview of 186 cases published during the last century. Acta Neurochir (2010) 152:749-61. DOI: https://doi.org/10.1007/s00701-009-0595-8
Biousse V, Newman NJ, Oyesiku NM. Precipitating factors in pituitary apoplexy. J Neurol Neurosurg Psychiatry 2001;71:542- 545 DOI: https://doi.org/10.1136/jnnp.71.4.542
Randeva HS, Schoebel J, Byrne J, et al. Classical pituitary apoplexy: clinical features, management and outcome. Clin Endocrinol 1999;51:181-8. DOI: https://doi.org/10.1046/j.1365-2265.1999.00754.x
Harris SM, Cannon JE, Carroll PV, Thomas SM. Pituitary apoplexy: two very different presentations with one unifying diagnosis. J R Soc Med Sh Rep 2010;1:53. DOI: https://doi.org/10.1258/shorts.2010.100073
Cho W, Joo S, Kim T, Seo B. Pituitary apoplexy presenting as isolated third cranial nerve palsy with ptosis: two case reports. J Korean Neurosurg Soc 2009;45:118-21. DOI: https://doi.org/10.3340/jkns.2009.45.2.118
Kashkouli MB, Khalatbari M, Yahyavi S, et al. Pituitary apoplexy presenting as acute painful isolated unilateral third cranial nerve palsy. Arch Iranian Med 2008;11:466-8.
Sowka JW, Gurwood AS, Kabat AG. Neuro-ophthalmic disease: Cranial nerve III palsy. Review of Optometry: The Handbook of Ocular Disease Management, 11th ed. April 15, 2009:50A-52A.
Kim SH, Lee KC, Kim SH. Cranial nerve palsies accompanying pituitary tumour. J Clin Neurosci 2007;14:1158-62. DOI: https://doi.org/10.1016/j.jocn.2006.07.016
Saul RF, Hilliker JK. Third nerve palsy: the presenting sign of a pituitary adenoma in five patients and the only neurological sign in four patients. J Clin Neuroophthalmol 1985;5:185-93.
Kobayashi et al. A possible mechanism of isolated oculomotor nerve palsy by apoplexy of pituitary adenoma without cavernous sinus invasion: a report of two cases. Acta Neurochir 2011;153:2453-6. DOI: https://doi.org/10.1007/s00701-011-1165-4
Dubuisson AS, Beckers A, Stevenaert A. Classical pituitary tumour apoplexy: clinical features, management and outcomes in a series of 24 patients. Clin Neurol Neurosurg 2007;109:63-70. DOI: https://doi.org/10.1016/j.clineuro.2006.01.006
Sibal L, Ball SG, Connolly V, et al. Pituitary apoplexy: a review of clinical presentation, management and outcome in 45 cases. Pituitary 2004;7:157-63. DOI: https://doi.org/10.1007/s11102-005-1050-3
Woo HJ, Hwang JH, Hwang SK, Park YM. Clinical outcome of cranial neuropathy in patients with pituitary apoplexy. J Korean Neurosurg Soc 2010;48:213-8. DOI: https://doi.org/10.3340/jkns.2010.48.3.213
Lethall RK, Jaspan T. A case of isolated third nerve palsy with pupil involvement. Br J Radiol 2000;73:569-70. DOI: https://doi.org/10.1259/bjr.73.869.10884760
Brisman M H Katz, Post KD. Symptoms of pituitary apoplexy rapidly reversed with bromocriptine. J Neurosurg 1996;85:1153-5. DOI: https://doi.org/10.3171/jns.1996.85.6.1153
De Araujo L C, Zapupulla RA, Quinonez R O, Noh J M. Pituitary adenoma presenting as post-traumatic oculomotor palsy: report of two cases. Neurosurgery 1979;4:427-30. DOI: https://doi.org/10.1227/00006123-197905000-00009
Chen HY, Tsai RK, Howng SL. Acute painful oculomotor nerve paresis caused by pituitary apoplexy—a case report. Kaohsiung J Med Sci 1999;15:437-40.
Lee C C, Cho A S, Carter W A. Emergency department presentation of pituitary apoplexy. Am J Emerg Med 2000;18:328-31. DOI: https://doi.org/10.1016/S0735-6757(00)90130-X
Rossitch E, Carrazana E J, Black PM. Isolated oculomotor nerve palsy following apoplexy of a pituitary adenoma. J Neurosurg Sci 1992;103-5.
Varma D, Tesha P, George N. Acute painful third nerve palsy: the sole presenting sign of a pituitary adenoma. Eye 2002;16:792-3. DOI: https://doi.org/10.1038/sj.eye.6700186
Maccagnan P, Macedo CL, Kayath MJ, et al. Conservative management of pituitary apoplexy: a prospective study. J Clin Endocrinol Metab 1995;80:2190-7. DOI: https://doi.org/10.1210/jcem.80.7.7608278
Gruber A, Clayton J, Kumar S, et al. Pituitary apoplexy: retrospective review of 30 patients—is surgical intervention always necessary? Br J Neurosurg 2006;20:379-85. DOI: https://doi.org/10.1080/02688690601046678