Designing a workshop for a temporal artery biopsy simulation
Article Sidebar
Main Article Content
Abstract
Purpose
To evaluate a wet-lab session designed to teach temporal artery biopsy (TAB) using simulation.
Methods
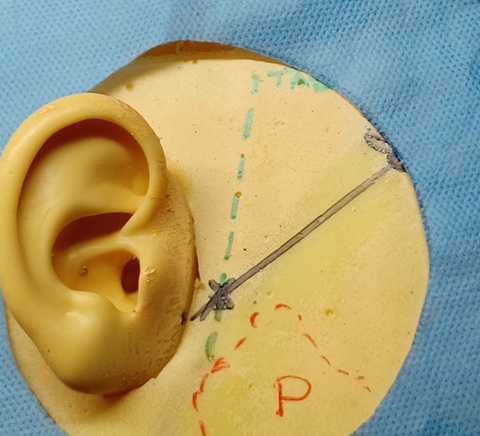
The Welsh Institute for Minimal Access Therapy Team (WIMAT) developed two simulation models using pig ureter for the temporal artery. The session consisted of consultant-led teaching on TAB surgical approaches, mapping the temporal artery with a Doppler device, and practical demonstrations with videos. Trainees performed two biopsies using the models under consultant supervision. Participants completed questionnaires to evaluate their pre- and post-session knowledge, understanding, and learning experiences. Three key areas of comparison were mapping the temporal artery, using an ultrasound doppler device, and performing a TAB.
Results
Seven specialist trainees (ST1-5) and 3 staff grade surgeons, supervised by 3 consultants, participated. Paired t test sampling showed statistically significant improvements in mapping the temporal artery (P = 0.0076), using an ultrasound Doppler device (P = 0.0002), and performing a TAB (P = 0.0002). Identified barriers included lack of knowledge, limited prior procedures, concern about damaging the facial nerve, and lack of senior support/supervision, which contributed to trainees’ apprehension about performing TAB.
Conclusions
This innovative teaching event offers a blueprint for medical training programs to improve TAB training. Modern surgical education benefits from wet labs with expert supervision.
Downloads
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.




References
Mackie SL, Dejaco C, Appenzeller S, et al. British Society for Rheumatology guideline on diagnosis and treatment of giant cell arteritis: executive summary. Rheumatology (Oxford) 2020;59:487-94. DOI: https://doi.org/10.1093/rheumatology/keaa475
Ing EB, Wang DN, Kirubarajan A, et al. Systematic review of the yield of temporal artery biopsy for suspected giant cell arteritis. Neuroophthalmology 2018;43:18-25. DOI: https://doi.org/10.1080/01658107.2018.1474372
Mollan SP, Paemeleire K, Versijpt J, et al. European Headache Federation recommendations for neurologists managing giant cell arteritis. J Headache Pain 2020;21:28. DOI: https://doi.org/10.1186/s10194-020-01093-7
Al-Mousawi AZ, Gurney SP, Lorenzi AR, et al. Reviewing the pathophysiology behind the advances in the management of giant cell arteritis. Ophthalmol Ther 2019;8:177-93. DOI: https://doi.org/10.1007/s40123-019-0171-0
Coath FL, Bukhari M, Ducker G, et al. Quality standards for the care of people with giant cell arteritis in secondary care. Rheumatology (Oxford) 2023;62:3075-83. DOI: https://doi.org/10.1093/rheumatology/kead025
Galloway GD, Klebe B, Riordan-Eva P. Surgical performance for specialties undertaking temporal artery biopsies: who should perform them? Br J Ophthalmol 2002;86:250. DOI: https://doi.org/10.1136/bjo.86.2.250
Rogers GM, Oetting TA, Lee AG, et al. Impact of a structured surgical curriculum on ophthalmic resident cataract surgery complication rates. J Cataract Refract Surg 2009;35:1956-60. DOI: https://doi.org/10.1016/j.jcrs.2009.05.046
Osei G, Rainsbury P, Morris D, et al. Temporal artery biopsy: time for a rethink on training? Eye (Lond) 2023;37:506-10. DOI: https://doi.org/10.1038/s41433-022-01963-1
Le KDR. Principles of effective simulation-based teaching sessions in medical education: a narrative review. Cureus 2023;15:e49159. DOI: https://doi.org/10.7759/cureus.49159
Kotsis SV, Chung KC. Application of see one, do one, teach one concept in surgical training. Plast Reconstr Surg 2013;131:1194-201. DOI: https://doi.org/10.1097/PRS.0b013e318287a0b3
Romero P, Gunther P, Kowalewski KF, et al. Halsted’s “see one, do one, and teach one” versus Peyton’s four-step approach: a randomized trial for training of laparoscopic suturing and knot tying. J Surg Educ 2018;75:510-5. DOI: https://doi.org/10.1016/j.jsurg.2017.07.025
Engels PT, de Gara C. Learning styles of medical students, general surgery residents, and general surgeons: implications for surgical education. BMC Med Educ 2010;10:51. DOI: https://doi.org/10.1186/1472-6920-10-51
Agha RA, Fowler AJ. The role and validity of surgical simulation. Int Surg 2015;100:350-7. DOI: https://doi.org/10.9738/INTSURG-D-14-00004.1
Lopez-Beauchamp C, Singh GA, Shin SY, et al. Surgical simulator training reduces operative times in resident surgeons learning phacoemulsification cataract surgery. Am J Ophthalmol Case Rep 2020;17:100576. DOI: https://doi.org/10.1016/j.ajoc.2019.100576
Ferris JD, Donachie PH, Johnston RL, et al. Royal College of Ophthalmologists’ National Ophthalmology Database study of cataract surgery: report 6. The impact of EyeSi virtual reality training on complications rates of cataract surgery performed by first and second year trainees. Br J Ophthalmol 2020;104:324-9. DOI: https://doi.org/10.1136/bjophthalmol-2018-313817
Staropoli PC, Gregori NZ, Junk AK, et al. Surgical simulation training reduces intraoperative cataract surgery complications among residents. Simul Healthc 2018;13:11-15. DOI: https://doi.org/10.1097/SIH.0000000000000255
Feudner EM, Engel C, Neuhann IM, et al. Virtual reality training improves wet-lab performance of capsulorhexis: results of a randomized, controlled study. Graefes Arch Clin Exp Ophthalmol 2009;247:955-63. DOI: https://doi.org/10.1007/s00417-008-1029-7
Daly MK, Gonzalez E, Siracuse-Lee D, et al. Efficacy of surgical simulator training versus traditional wet-lab training on operating room performance of ophthalmology residents during the capsulorhexis in cataract surgery. J Cataract Refract Surg 2013;39:1734-41. DOI: https://doi.org/10.1016/j.jcrs.2013.05.044