Impact of phacoemulsification on posterior vitreous detachment formation in eyes with vitreomacular traction
Article Sidebar
Main Article Content
Abstract
Purpose
To investigate the impact of phacoemulsification on posterior vitreous detachment formation in eyes with vitreomacular traction (VMT) with or without macular holes.
Methods
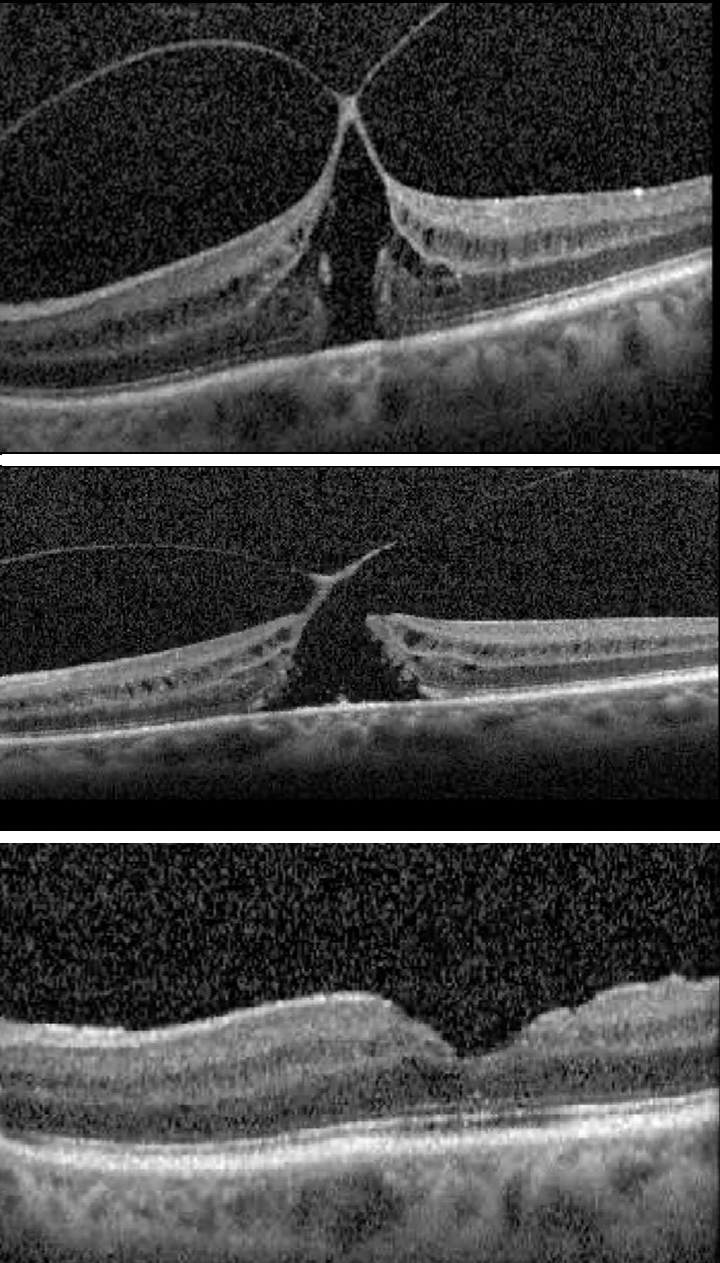
A retrospective search of the medical records was conducted to identify patients with VMT who underwent cataract surgery at Mass Eye and Ear from 2016 to 2021. Patient demographics, ocular comorbidities, and clinical characteristics were extracted from the record, and optical coherence tomography images were assessed to confirm VMT and the presence of a lamellar or full-thickness macular hole (FMTH). Patients who underwent vitrectomy prior to cataract surgery were excluded.
Results
A total of 22 patients (15 women [68%]) met inclusion criteria (average age, 71 years). Fifteen eyes had an associated epiretinal membrane (63%), 7 had a lamellar hole (29%), and 8 had an FTMH (33%). Epiretinal membrane was present in 3 of 7 eyes with lamellar holes (43%) and 4 of 8 with a FTMH (50%). No eyes developed a complete posterior vitreous detachment following phacoemulsification. In 2 cases, there was progression of the macular hole stage following phacoemulsification. Ten eyes underwent subsequent pars plana vitrectomy (PPV). There was no statistically significant difference in visual acuity between eyes pre- and post-phacoemulsification; however, there was a statistically significant improvement in visual acuity pre- and post-PPV.
Conclusions
Unlike other studies, in this case series of 24 eyes with VMT or VMT with holes, no cases of full posterior vitreous detachment occurred following unremarkable phacoemulsification or YAG capsulotomy.
Downloads
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.




References
Duker JS, Kaiser PK, Binder S, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology 2013;120:2611-19. DOI: https://doi.org/10.1016/j.ophtha.2013.07.042
Rodman JA, Shechtman D, Sutton BM, Pizzimenti JJ, Bittner AK; VAST Study Group. Prevalence of vitreomacular adhesion in patients without maculopathy older than 40 years. Retina 2018;38:2056-63. DOI: https://doi.org/10.1097/IAE.0000000000001792
Menzler J, Neubauer AS, Haritoglou C, Jackson TL. Incidence and prevalence of vitreomacular traction with and without macular hole in Germany. Clin Ophthalmol 2019;13:177-88. DOI: https://doi.org/10.2147/OPTH.S188704
Hayashi S, Yoshida M, Hayashi K, Tsubota K. Progression of posterior vitreous detachment after cataract surgery. Eye (Lond) 2022;36:1872-7. DOI: https://doi.org/10.1038/s41433-021-01732-6
Mantopoulos D, Prenner JL, Patel VK, et al. The effect of elective cataract extraction by phacoemulsification in eyes with vitreomacular traction syndrome. Retina 2021;41:75-81. DOI: https://doi.org/10.1097/IAE.0000000000002785
Carpineto P, Ciciarelli V, Borrelli E, Aharrh-Gnama A, Mastropasqua R. Epiretinal membrane in eyes with vitreomacular traction. Retina 2019;39:1061-5. DOI: https://doi.org/10.1097/IAE.0000000000002546
Panagiotidis D, Karagiannis D, Theodossiadis P, et al. Cataract-related acute vitreomacular traction syndrome. Eur J Ophthalmol 2011;21:20-3. DOI: https://doi.org/10.5301/EJO.2010.521
Park JH, Yang H, Kwon H, Jeon S. Risk factors for onset or progression of posterior vitreous detachment at the vitreomacular interface after cataract surgery. Ophthalmol Retina 2021;5:270-8. DOI: https://doi.org/10.1016/j.oret.2020.07.017
Sheard RM, Goodburn SF, Comer MB, Scott JD, Snead MP. Posterior vitreous detachment after neodymium:YAG laser posterior capsulotomy. J Cataract Refract Surg 2003;29:930-4. DOI: https://doi.org/10.1016/S0886-3350(02)01837-0