Infectious keratitis following laser in situ keratomileusis (LASIK)
Article Sidebar
Main Article Content
Abstract
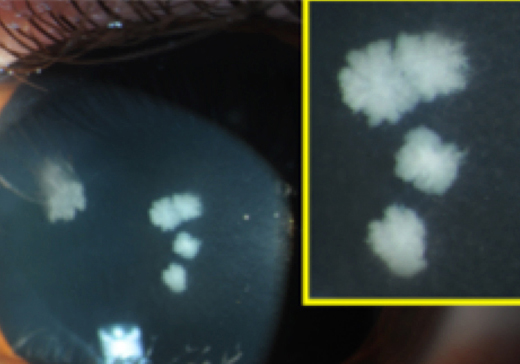
A 22-year-old healthy man who had undergone uncomplicated LASIK 3 weeks prior to presentation at an outside institution presented to the Vanderbilt Eye Institute with 3 days of bilateral blurry vision, photophobia, and pain. The patient was using topical steroids. He denied a history of trauma or contact with organic matter. On examination, best-corrected visual acuity was 20/40 in the right eye and 20/70 in the left. There were multifocal feathery infiltrates within the cornea under the partial-thickness LASIK flaps bilaterally (A-B). The corneal flaps were lifted to culture and irrigate the interface, and moxifloxacin and trimethoprim/polymyxin b were initiated. Cultures grew Mycobacterium chelonae on Löwenstein-Jensen medium, and the antibiotics were switched to amikacin and clarithromycin. Prednisolone acetate was subsequently added. At 8 weeks’ follow-up, the keratitis had fully resolved (C-D), with best-corrected acuity of 20/25 in the right and 20/30 in the left eye. Atypical mycobacteria are a major cause of post-LASIK infections and aggressive treatment directed against these organisms must be considered in all cases of post-LASIK infection. If the infection cannot be controlled with flap irrigation and medical therapy, flap amputation or corneal transplantation should be considered.
Downloads
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.