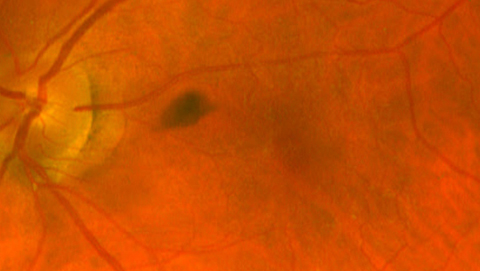
Hollenhorst plaque in left superior temporal cilioretinal arterial bifurcation
Article Sidebar
Main Article Content
Abstract
An 81-year-old man with noncontributory ocular history presented at the UVA Department of Ophthalmology Walk-in Clinic for sudden-onset transient scotoma in the left eye of 2 hours’ duration. He was found to have a Hollenhorst plaque at the left superior temporal cilioretinal arterial bifurcation (A-B). On examination, visual acuity was 20/20 in the left eye and 20/25 in the right eye. Fundus examination was otherwise normal, and there was no evidence of retinal tears or detachment, retinal ischemia, or venous channel irregularity. He was referred to cardiology for a follow-up carotid doppler and transthoracic echocardiogram, which revealed moderate stenosis of the left carotid artery likely associated with a cholesterol plaque. At 6-months’ follow-up, the patient remained without visual symptoms, and examination revealed that the Hollenhorst plaque had disappeared, with attenuation of the distal cilioretinal artery (C). At the most recent follow-up visit, several years after the first incident, he was found to have a recurrence of the Hollenhorst plaque in the inferior disc margin of the same eye (D).
Downloads
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.