Ocular tilt reaction
Article Sidebar
Main Article Content
Abstract
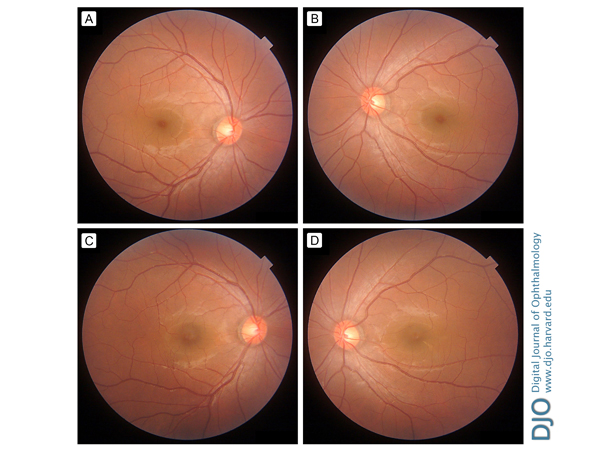
A 30-year-old man presented to the ophthalmologic clinic at Jichi Medical University with sudden-onset vertical and torsional diplopia. Concomitant skew deviation with right hypertropia was observed. Funduscopy revealed that the fovea was located above the lower edge of the optic disc in the right eye; incyclotorsion was present (A). Conversely, the fovea was located below the lower edge of the optic disc in the left eye; excyclotorsion was present (B). The patient was diagnosed with ocular tilt reaction (OTR). Neurological examination was unremarkable. Cranial magnetic resonance imaging demonstrated no abnormalities and no evidence of acute ischemia, demyelination, or vestibular nerve abnormality. The patient was followed, without treatment. One month later, his diplopia had disappeared. Incyclotorsion in the right eye and excyclotorsion in the left eye were also improved (C-D). OTR consists of ocular torsion, skew deviation, and tilt of subjective visual vertical with or without head tilt. It indicates a unilateral deficit of otolithic input or a unilateral lesion of the graviceptive brainstem pathway from the vestibular nucleus to the rostral midbrain, which crosses the midline at the pontine level. Although vertical and torsional diplopia was the only symptom in this patient, we speculate that OTR can result from a subclinical peripheral vestibulopathy affecting the otolith-ocular pathways.
Downloads
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.